
Background
In the intensive care unit (ICU), providing life-saving treatment is the primary goal. However, for many patients facing the end of life, aggressive treatments might prolong suffering without improving outcomes. Often, the patient’s wishes for end-of-life care are unknown, leaving healthcare providers and families to make difficult decisions. This situation highlights the critical need for effective Cares Tool For End Of Life, specifically communication strategies to guide these challenging conversations.
Recognizing this gap, various communication tools have been developed to assist families and clinicians in end-of-life decision-making in the ICU. These tools range from structured meeting plans to decision aids, aiming to facilitate discussions about goals of care, code status, and the appropriateness of life-sustaining treatments. To understand the effectiveness of these cares tool for end of life, a comprehensive review was conducted to analyze existing research. This article summarizes the findings of a systematic review that investigated the impact of structured communication tools on end-of-life decision-making in the ICU compared to usual care. The review focused on key outcomes such as documented goals of care discussions, code status, and decisions regarding life-sustaining treatments.
Methods
To gather evidence, a thorough search was conducted across major medical databases, covering studies up to July 2014. The search included databases like MEDLINE, Embase, CINAHL, ERIC, and Cochrane, ensuring a broad range of relevant literature was captured. Researchers independently screened thousands of articles to identify studies that met specific criteria. These criteria focused on studies evaluating communication tools designed to aid end-of-life decision-making in adult ICU patients. The quality of the included studies was assessed using established tools, ensuring the reliability of the review’s findings. Where possible, data from similar studies were combined to provide a more robust estimate of the effect of communication tools. The overall quality of the evidence for each outcome was evaluated using the GRADE system, which assesses the certainty of research findings.
Results
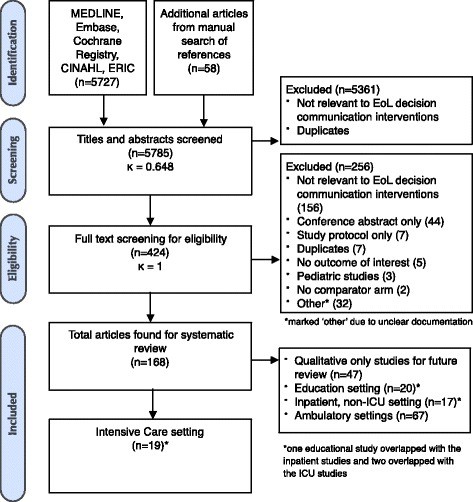
The extensive search and screening process resulted in the review of over 5,700 abstracts, leading to the identification of 168 relevant articles, with 19 specifically focusing on the ICU setting. The analysis of these ICU studies revealed that using communication tools significantly increased the documentation of goals-of-care discussions.
Study selection process flowchart, detailing the stages from initial database searches to final inclusion of studies for systematic review, highlighting the number of articles screened, assessed for eligibility, and included in the analysis.
However, the use of these cares tool for end of life did not show a significant impact on documenting code status or decisions to withdraw or withhold life-sustaining treatments. Interestingly, the review found that communication tools were associated with a reduction in healthcare resource utilization. This reduction was observed in measures such as the duration of mechanical ventilation, length of ICU stay, and healthcare costs.
Primary Outcomes in Detail
The primary outcomes examined in this review were crucial indicators of end-of-life care quality. The analysis showed that communication tools had a notable positive effect on the documentation of goals-of-care discussions. Specifically, the use of these tools more than tripled the likelihood of these vital discussions being formally recorded in patient charts.
This finding is significant because documented goals of care discussions ensure that patient preferences and values are considered in treatment decisions. However, while communication tools improved documentation of these discussions, they did not translate into a significant change in code status documentation. The review found no significant difference in the rate of documented code status, including “Do Not Resuscitate” (DNR) orders, between groups using communication tools and those receiving usual care.
Similarly, the analysis revealed that communication tools did not significantly affect decisions to withdraw or withhold life-sustaining treatments. There was no statistically significant difference in the proportion of patients for whom decisions were made to limit aggressive treatments between the intervention and control groups.
Secondary Outcomes: Resource Utilization and More
Beyond the primary outcomes, the review explored secondary outcomes to understand the broader impact of cares tool for end of life. One key area was healthcare resource utilization. The analysis indicated that communication tools were associated with a significant decrease in several measures of resource use. Patients in groups using communication tools experienced a reduction in the duration of mechanical ventilation by an average of almost two days.
Furthermore, the length of stay in the ICU was also reduced by over a day in groups utilizing communication tools.
This pattern of reduced resource utilization extended to financial costs. The review found evidence suggesting that the use of communication tools led to lower healthcare costs.
However, it’s important to note that the quality of evidence supporting these findings on resource utilization, like the primary outcome findings, was rated as very low. Other secondary outcomes explored included patient and family satisfaction, knowledge about end-of-life care, and quality of communication. Due to limited data and study heterogeneity, the review could not draw firm conclusions about the impact of communication tools on these aspects.
Discussion
The findings of this review highlight a critical area in ICU care: end-of-life decision-making. While the use of structured communication tools shows promise in improving documentation of goals-of-care discussions, the overall quality of evidence is low to very low. This means that while these cares tool for end of life may be beneficial, further high-quality research is needed to confirm their effectiveness.
The lack of significant impact on code status and decisions to withdraw or withhold treatments, despite increased documentation of discussions, raises important questions. It’s possible that the existing studies lacked the statistical power to detect subtle but real effects, or that the tools themselves need refinement to more effectively translate discussions into concrete decisions and actions. Another consideration is the timing of interventions. Intervening earlier in a patient’s care trajectory, before ICU admission, might be more impactful in shaping end-of-life care plans.
The observed reduction in healthcare resource utilization associated with communication tools is intriguing. It suggests that these tools might lead to more efficient care, potentially by facilitating earlier transitions to palliative or comfort-focused approaches when appropriate. However, the mechanisms behind this reduction require further investigation. It’s crucial to understand whether this is due to actual changes in treatment decisions or other factors related to communication strategies.
Conclusion
This systematic review provides a valuable overview of the current evidence on communication tools for end-of-life decision-making in the ICU. While structured communication tools may improve the documentation of crucial conversations and potentially reduce resource use, the evidence is currently of low to very low quality. Therefore, there is a clear need for more robust, high-quality randomized controlled trials to definitively determine the impact of these cares tool for end of life. Future research should focus on well-designed studies that evaluate patient-level, family-level, and system-level outcomes. Specifically, studies should examine the impact of communication tools on patient satisfaction, family well-being, healthcare costs, and the alignment of care with patient wishes. Ultimately, enhancing end-of-life care in the ICU requires a continued commitment to research and the implementation of evidence-based strategies, including effective communication tools.
Key messages
- Research on structured communication tools in ICU end-of-life care is growing.
- Evidence for increased documentation of goals-of-care discussions is present, but of low quality.
- Impact on code status documentation and treatment withdrawal decisions is not significantly demonstrated.
- Healthcare resource utilization may be reduced with communication tools, but evidence quality is low.
- More high-quality studies are essential to validate the benefits and optimize the use of cares tool for end of life in the ICU.